Are There All-Virtual First Aid, CPR, and AED Certification Classes?
The COVID-19 pandemic has led to a surge in demand for all-virtual training programs. Before the pandemic, online courses could not issue first aid, CPR, or AED certificates unless they were complemented by hands-on skills practice with an instructor. But social distancing rules and the ubiquity of web-conferencing have persuaded regulators to approve remote skills assessments.
Although they were designed to minimize the risk of spreading COVID-19, all-virtual courses are likely to stay popular even beyond the pandemic. Training providers and clients alike have found that virtual learning can solve logistical problems, especially since many employees maintain different remote and in-office schedules.
Most students spend significantly less time on computer-based lessons than instructor-led classes. However, studies are finding that virtual courses are actually better at teaching life-saving skills. Compared to students who learn in traditional classrooms, virtual students are better at performing CPR and retain their knowledge for longer, making them more confident and willing to rescue someone with a medical emergency.
History & Background
Blended Learning
The Occupational Safety and Health Administration’s (OSHA) general industry standard requires workplaces without a hospital or emergency care center within three to four minutes to have employees trained to provide first-aid, which includes CPR. OSHA relies on two non-profit health organizations: the American Red Cross and the American Heart Association to set the standards for first-aid, CPR, and AED training. These organizations change the curriculum based on the latest medical and educational research.
However, even after online and computer-based programs started becoming the standard for state-mandated workplace training such as sexual harassment and discrimination, OSHA affirmed that first-aid training could not be completed online. Learning emergency procedures such as CPR requires trainees to “develop hands-on skills through the use of mannequins and partner practice,” as well as the “verification of competent skill performance by a qualified trainer.”
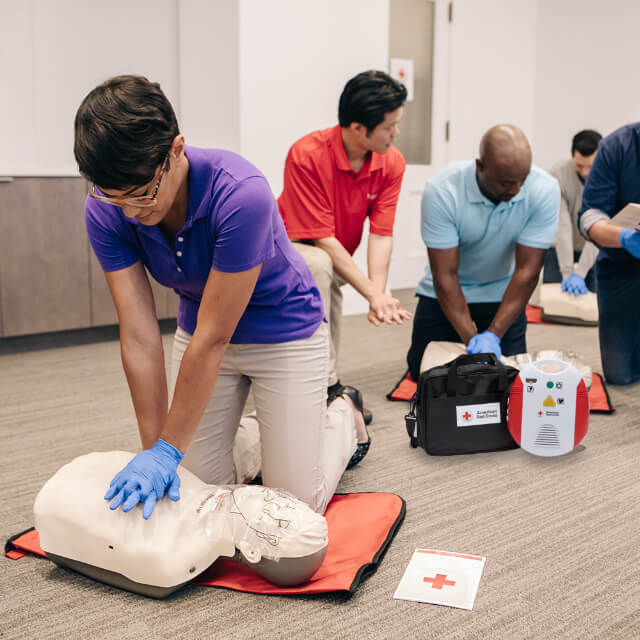
Many certified training providers started to offer blended learning courses, which combine a computer-based instructional component and an in-person, hands-on skills assessment with a manikin and instructor. Blended certification programs have been around for over a decade. For example, the American Red Cross started to offer them as early as 2005.
COVID-19
After COVID-19, both in-person and blended certification courses became unsafe. Online lessons remained a viable alternative because it did not require instructors and students to be in the same classroom. However, the hands-on training would still have required instructors and students to work face-to-face and without masks when practicing CPR.
With blended programs on pause, workers across the U.S.–including first responders–had no way to renew their compliance certificates. In March 2020, the American Heart Association gave up to a six-month extension on expiring CPR certificates for instructors and health professionals. Many hospitals were overwhelmed with COVID cases, and the American Heart Association wanted medical staff to prioritize treating patients.
Virtual Skills Training
The following month, the American Red Cross published its “Interim Virtual Skills Training” guidelines, which adapted their first aid, CPR, and AED programs to meet social distancing requirements. After this pivotal moment, people could start getting certified or recertified by taking all-virtual courses.
“The health and safety of participants and instructors is always our top priority,” says Jody P. Wacker, VP of Marketing for American Red Cross Training Services. “Remote skills assessment guidance was created for those students and partners that wanted to be able to safely and effectively attend or offer a skills session without being in-person.”
Under these guidelines, each participant, including the instructor, is required to work in a separate room. The all-virtual courses achieve this by replacing the close-quarters skills assessment with a remote setup where the instructor can observe and comment on a student’s hands-on practice using web-conference software such as Zoom and Microsoft Teams.
“Several organizations have implemented virtual or remote skills assessments,” explains Wacker. “The Red Cross along with our Scientific Advisory Council crafted very detailed processes to ensure skills were measured correctly.”
For example, students must position and angle laptop webcams so that instructors can get a clear view of the student, manikin, AED trainer, and/or first aid supplies. Web conferences must be conducted on high-speed internet to ensure seamless observation and communication through video and audio channels. The manikin itself must have “a feedback device that provides real-time audio and/or visual feedback on adequacy of compression rate and depth” such as a clicker or lights.
Personal Manikins
In addition to virtual skills assessments, the American Red Cross also requires that shared manikins are sanitized between students and that each student uses a breathing barrier. Also, every student and instructor must have their own disposable equipment such as bandages, gloves, and lung bags.
Some courses have started to incorporate personal manikins, [such as the American Heart Association’s CPR Anytime manikin]. Originally designed for at-home training, these personal manikins are cost-effective enough to issue to individual students, eliminating the decontamination process, which could be difficult to navigate. Although the American Red Cross intended to publish a Manikin decontamination protocol, it ultimately deferred to “CDC guidance, the manikin manufacturer’s directions, and the process recommended by the cleaning product manufacturers.”
Because these manikins are inflatable, they come in a compact package, making them easy to ship and store. With the bulkier, more expensive models, even though COVID safety protocols and all-virtual courses required instructors and students to remain in separate rooms, instructors would still have to travel to the workplace just to deliver and retrieve the manikin. In lieu of an employee-volunteer trained in decontamination procedures, instructors would also have to stay on site to sanitize shared manikins between individual skill assessments.
By shipping all required gear (and using an online registration process), instructors can teach the course without stepping foot in the client’s workplace. A fully remote program gives employees even more flexibility, as they no longer have to schedule the skills assessment for when the instructor is at the workplace. Remote employees can fully complete the course from work or from home, so their training is up-to-date if and when they return to the office–or in case they have to rescue a family member at home.
Studies: Virtual Training Beyond COVID
In addition to the logistical benefits, studies are showing that virtual courses are actually better at teaching the material. Online lessons allow students to work at their own pace. The American Red Cross found that healthcare providers who used online courses spent 40 percent less time than those in traditional classrooms. In some courses, students have the option to test out of sections.
One might think that less time spent in the instructional component might lower proficiency and retention rates, but research comparing computer-based to in-person learning have shown the opposite.
A 2010 study compared the performance outcomes of 71 volunteer laypersons, who learned CPR and first-aid from either an in-person or blended learning course. On average, online students spent 3 hours on coursework, almost a third of the time spent in the 8-hour instructor-led classes. However, data taken from the manikins showed that the online students outperformed their counterparts in the CPR skills assessment.
In 2021, researchers investigated whether hybrid and all-online CPR classes could be a viable alternative to in-person classes during the pandemic. They analyzed 20 studies from around the world that were conducted between 1995 and 2010 on various groups: from school children and high-schoolers to laypersons and medical students. These studies compared the skills performance and knowledge of people without previous CPR training after they had taken an in-person, hybrid, or all-online course.
Overall, the studies found that the hybrid or all-online group “performed better in assessing scene safety, calling for help, response time including initiating first rescue breathing, adequate ventilation volume, compression rates, shorter hands-off time, confidence, willingness to perform CPR, ability to follow CPR algorithm, and equivalent or better knowledge retention than standard teaching methodology.”
The 11 studies that included all-online classes used manikins with a built-in audio feedback mechanism. Students practicing on these manikins had more correct hand positioning and better compression rates than the instructor-led students.
“Interactive mannikins that measure your skills continue to be developed,” says Wacker. “These types of tools easily support virtual skills testing.”
Computer-based teaching also improves retention rates by 25 to 60 percent, according to a 2013 study by the Research Institute of America. Students using e-learning can work at their own pace: they can revisit difficult material and skim through easier or familiar information. Breaking up content prevents brains from being overloaded, making it easier to transfer new information from working memory to long-term memory.
As of March 2022, there have been almost 450 million COVID-19 cases and six million deaths worldwide. These stark numbers do not even account for health outcomes that were adversely affected by the pandemic’s secondary impacts.
Cardiac arrest is still the leading cause of death worldwide, accounting for 17 million or 25 percent of deaths each year. Out-of-hospital cardiac arrests occur in over 40 out of 10,000 people. To put this into perspective, about 7 out of 10,000 people have died from COVID-19. If a bystander performs CPR before EMS arrives, the victim’s survival rate increases three-fold.
““The pandemic continues to change the way many of us do business and training is included in that,” says Wacker. “One of the benefits of remote verification is that a student continues to practice the necessary skills for lifesaving.”
While we have to prioritize minimizing the spread of COVID-19, it is also important to adapt our environments and behaviors to reduce the pandemic’s secondary impacts. We have many pre-COVID technologies at our disposal: from portable air purifiers that filter airborne pathogens in offices and healthcare clinics to web-conferencing software that can help people work from home or learn how to respond to life-threatening emergencies. In many cases, our ability to move forward will be determined by our willingness to rewrite established rules and finding innovative ways to integrate existing technologies.
OSHA. Clarification of “in near proximity” and OSHA’s discretion in enforcing first aid requirements in particular cases. Occupational Safety and Health Administration: Standard Interpretations. 1910.151. MAmerican Red Crossh 23, 2007. https://www.osha.gov/laws-regs/standardinterpretations/2007-03-23
OSHA. First Aid Programs. Occupational Safety and Health Administration: Medical and First Aid. Accessed Feb 15, 2022. https://www.osha.gov/medical-first-aid/programs
Merchant, R.M., et. al. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. Oct 21, 2020. https://doi.org/10.1161/CIR.0000000000000918
OSHA. Clarification of OSHA training requirements for basic first aid and cardiopulmonary resuscitation (CPR). Occupational Safety and Health Administration: Standard Interpretations. 1910.151. Aug 2, 2012. https://www.osha.gov/laws-regs/standardinterpretations/2007-03-23
American Heart Association. Interim Guidance on Card Extensions during COVID19 Outbreak. American Heart Association: CPR & Emergency Cardiovascular Care. MAmerican Red Crossh 31, 2020. https://cpr.heart.org/-/media/cpr-files/resources/covid-19-resources-for-cpr-training/covid19-statement_card-extensions_update-33120.pdf
American Red Cross. Interim Virtual Skills Training. American Red Cross COVID-19 Guidance: First Aid/CPR/AED. April 16, 2020. https://American Red Cross-phss.my.salesforce.com/sfc/p/#d0000000bxKz/a/3o000001WYjw/fFpJ7gMELPAR.QJZ68.YQNvBpxtRvU9k351u2btZOCw
American Heart Association. Adult & Child CPR Anytime Kits. American Heart Association: CPR & First Aid: Emergency Cardiovascular Care. Accessed Feb 20, 2020. https://cpr.heart.org/en/courses/adult-and-child-cpr-anytime-training-kits
American Red Cross. Coronavirus (COVID-19): Prevention & Safety Information for Students. American Red Cross: Health & Safety Training in the News. August 30, 2021. https://www.redcross.org/take-a-class/in-the-news/coronavirus-prevention-information-for-students
American Red Cross. Blended Learning Benefits Your Organization. American Red Cross Training Services.
Cason, C., & Stiller, J. (2010). Performance outcomes of an online first aid and CPR course for laypersons. Health Education Journal, 70(4), 458-467. doi: http://dx.doi.org/10.1177/0017896910379696
Ali, D. M., Hisam, B., Shaukat, N., Baig, N., Ong, M., Epstein, J. L., Goralnick, E., Kivela, P. D., McNally, B., & Razzak, J. (2021). Cardiopulmonary resuscitation (CPR) training strategies in the times of COVID-19: a systematic literature review comparing different training methodologies. Scandinavian journal of trauma, resuscitation and emergency medicine, 29(1), 53. https://doi.org/10.1186/s13049-021-00869-3
Pappas, Christopher. “Top 10 e-Learning Statistics for 2014 You Need To Know”. eLearning Industry. December 1, 2013. https://elearningindustry.com/top-10-e-learning-statistics-for-2014-you-need-to-know
Guyan, Matthew. “5 Ways to Reduce Cognitive Load in eLearning.” eLearning Industry. November 1, 2013. https://elearningindustry.com/5-ways-to-reduce-cognitive-load-in-elearning

{kind=link}